Development and Assessment of Learners’ Experiences with a Virtual Reality Learning Platform: Constructivist and Experiential Learning Pedagogies in Master of Physical Therapy Curriculum
Stacey Lovo, University of Saskatchewan, Canada
Don Leidl, University of New Brunswick, Canada
Kendra Usunier, University of Saskatchewan, Canada
Teresa Paslawski, University of Saskatchewan, Canada
Mike Wesolowski, University of Saskatchewan, Canada
Arjun Puri, University of Calgary, Canada
Valerie Caron, University of Saskatchewan, Canada
Soo Kim, University of Saskatchewan, Canada
Copyright 2024 The Author(s). CC-BY-NC-ND License 4.0 This is an open access work distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits copy and redistribution with appropriate credit. This work cannot be used for commercial purposes and cannot be distributed if the original material is modified.
Abstract
Teaching competencies for psychomotor skill development for manual handling techniques in the cervical regions is necessary for safe practice in physiotherapy. However, grasping anatomy and palpation can be challenging for students, and practice in the lab can lead to discomfort for students. To facilitate teaching and learning of this complex skill, we worked in partnership with a virtual reality (VR) industry partner who developed a customized VR application focusing on transverse ligament stress testing for manual therapy skills for Master of Physical Therapy (MPT) students. In this scholarship of teaching and learning (SoTL) project, eight MPT students participated in the evaluation of an innovative VR learning experience for manual therapy in the cervical spine. Students’ learning experiences with the custom virtual reality learning application were assessed using an observational study design with semi-structured interviews. Interview questions aligned with constructs that are recommended to assess learners’ attitudes toward VR environments. Student participants appreciated the usefulness of the application for studying and practicing the transverse ligament stress test and provided recommendations for enhancing the learning experience.
Keywords: constructivist learning perspectives, experiential learning, virtual reality (VR), psychomotor skills, physical therapy, cervical spine, transverse ligament
Introduction
Several factors present challenges for Master of Physical Therapy (MPT) students when learning the transverse ligament stress test of the cervical spine with traditional teaching approaches. First, the anatomy of the craniovertebral (CV) region, which includes the occiput, atlas (C1), axis (C2), and supporting ligaments, is complex. The anatomy of the CV region is unique compared to other parts of the spine and can be more challenging for students to learn. Although review of the regional anatomy is provided, the two-dimensional (2D) images from anatomy textbooks as well as three-dimensional (3D) plastic models, void of any of the overlying soft tissue structures, are passive and lack experiential affordances (Estai &Bunt, 2016). Second, the CV region is small and deep to the muscles. For novice students who are still developing psychomotor skills for palpation, which is dependent on sound anatomical knowledge, navigating the region with their hands can not only be frustrating, but can also lead to discomfort and pain for their peers. Instructors have long noted frequent anecdotal reports of neck pain, soreness, headaches, occasional dizziness, and even migraines among students after having their peers practice the ligament test on them. Compounding these factors, learning time in the lab is limited in a tight curriculum, and opportunities for distributed practice during which to gain confidence and consolidate knowledge and skills in a safe environment may not be adequate.
A custom virtual reality (VR) application that affords students repeated opportunities for guided training of the ligament test in a safe and immersive environment and allows for adequate self-guided visualization of the relevant anatomy in 3D could mitigate challenges faced in MPT programs. Thus, the purpose of the project was two-fold. The first purpose was to develop a custom immersive VR application that could be used as a learning tool for MPT students to supplement traditional teaching methods of the transverse ligament stress test. This paper provides a descriptive account of this process and the pedagogical considerations that guided the design and methodology. The second purpose was to evaluate a pilot whereby students could experience the new learning tool. The observational pilot study is described and the impact on teaching and learning are discussed. This study responds to the following research question: What is the experience of MPT students using a custom VR learning platform for transverse ligament stress testing in the upper cervical spine?
LITERATURE REVIEW ON VR IN HEALTH SCIENCE EDUCATION
Virtual reality (VR) creates the perception of being physically present in a fully digital world and has been used in education for over 30 years to augment the teaching of a subject or topic. It allows an individual to experience and interact with a 3D digital environment for many purposes, including to gain practical understanding of concepts (Zhao et al., 2020). Virtual reality applications can enable varying degrees of immersion, from simple observation of a 360-degree video to complex and fully interactive 3D digital environments (Huang & Liaw, 2018). Higher levels of immersion, where the learners’ senses are fully immersed in a virtual environment, have been associated with increased engagement and motivation (Huang &Liaw, 2018). A VR environment is often explored by using a VR head-mounted display and input devices such as hand controllers (Moro et al., 2017).
In the education of health professionals, such as physical therapists, nurses, and doctors, VR can facilitate diverse forms of immersive learning (Kyaw et al., 2019). A common application for VR is in the teaching of anatomy. This type of education is considered a visual science and is a cornerstone for health profession education (Turney, 2007). Anatomy is not only important in gaining knowledge of the different structures of the human body, but also to appreciate the spatial relationships amongst these structures (Miller, 2000). As such, it is not surprising to see the uptake of VR among anatomy educators (Codd & Choudhury, 2011; Nicholson et al., 2016).
In recent reviews, the use of VR to enhance visualization of anatomy in 3D was evaluated (Moro et al., 2017; Zhao et al., 2020). When the educational effectiveness of VR in anatomy education was compared with other traditional methods (i.e., use of 2D images from textbooks), findings suggested VR could potentially improve the effectiveness of student learning. Although test performance was not found to be significantly enhanced by VR, the review and meta-analysis by Zhao et al. (2020) found that VR can be a viable alternative to traditional teaching methods and importantly that students’ interest in learning via VR methods is greater than with conventional or e-learning methods.
Other common uses of VR in health professions education have been for training of technical competencies, particularly in surgical simulations for medical education and psychomotor skill acquisition (Jiang et al., 2022). In recent years, there has been a surge of research investigating the efficacy of different VR applications developed to assist medical trainees in honing laparoscopic and orthopedic surgical skills (Banaszek et al., 2017; Brinkmann et al., 2017; Rahm et al., 2018; Zhang et al., 2013). Huang & Liaw (2018) and Sultan et al. (2019) noted that the use of VR to teach and practice clinical skills to decrease the risks of causing “harm” to patients, other students, or standardized patient actors is increasing. In a systematic review by Mao et al. (2021), immersive VR was found to improve surgical skill acquisition compared to non-VR training. Improvements in accuracy and time to complete skills were among some of the educational benefits. Although the majority of evidence for efficacy of VR training on the development of psychomotor skills has been for trainees who were further along in their training (i.e., medical residents), variations in efficacy between residents working on higher-level competency milestones and medical students working on beginner and intermediate-level competency milestones do not seem to be present.
Despite the interest and increased use of VR to augment the teaching of anatomy and to facilitate development of students’ psychomotor skills, as seen in medical, nursing, and dental education (Di Vece et al., 2021; Rourke, 2020; Zitzmann et al., 2020), VR research specific to physical therapy and other rehabilitation training and curricula is limited. Judd et al. (2021) recently presented the development of a VR application designed to facilitate learning and practicing of movement analysis skills. They also explored student reactions and attitudes toward use of the application. Hartstein et al. (2022) describe the development of a VR experience focused on promoting clinical decision-making and explore student and faculty experience with the VR. To our knowledge, however, there have not been any studies to date describing the design or application of VR to facilitate psychomotor skill development for ligamentous stress testing in physical therapy programs.
LEARNING THEORY AND FRAMEWORK CONSIDERATIONS FOR VIRTUAL REALITY
As VR can provide students with the opportunity to practice skills and techniques in a real-world setting, it is an ideal technology to foster experiential learning. Experiential learning theory defines learning as “the process whereby knowledge is created through the transformation of experience. Knowledge results from the combination of grasping and transforming experience” (Kolb, 1984). For experiential learning to occur, it should include these elements: 1) reflection, critical analysis, and synthesis; 2) opportunities for students to take initiative, make decisions, and be accountable for results; 3) opportunities for students to engage intellectually, creatively, emotionally, socially, or physically; and 4) a safe environment to learn from natural consequences, mistakes, and successes (Andresen et al., 2020; McCarthy, 2010). Thus, when a VR learning environment is carefully planned to include the elements outlined above, educators can leverage VR technology to build confidence and competency, especially for high-risk skills or skills that can cause discomfort or harm to patients or peers (Smith & Crocker, 2017).
Despite the rapid growth and use of VR in education, there is a lack of studies that describe the learning theories used to guide development and assessment of student learning so that it can be adapted or implemented into existing curricula (Huang & Liaw, 2018). To better understand students’ learning in VR environments, mounting research suggests that constructivist principles are paramount in both the design of the platform and assessment of students’ experiences (Huang et al., 2010). Within a constructivist paradigm, emphasis on the active role of the learner in building their own understanding is a key principle (Dewey, 1916). Thus, real-life contexts and problems are valuable educational experiences. Fundamental underpinnings of this paradigm also include the notions that knowledge is constructed and not passively absorbed and that a learner’s previous knowledge helps to construct new knowledge (Phillips, 1995). Virtual reality can be an excellent teaching tool in a constructivist classroom as it allows learners to interact and “feel” the content, which can help bridge the divide between theoretical learning in a classroom setting and real-life application of knowledge in a VR setting (Huang &Liaw, 2018).
Teachers and researchers can assess learners’ experiences and the educational value of a VR learning tool by applying the constructs within the technology acceptance model (TAM) (F. D. Davis, 1989). According to the TAM, the primary factors influencing an individual’s intention to use innovative technology such as VR are 1) perceived ease of use and 2) perceived usefulness (A. J. Davis et al., 1993). Perceived ease of use can be defined as the degree to which a learner believes that using a learning system would be effortless and perceived usefulness as the degree to which a learner believes that using a learning system would be beneficial to their learning (F. D. Davis, 1989; Huang & Liaw, 2018). Questions designed to capture learners’ attitudes about these constructs can help evaluate a learner’s overall motivation and intention to use a VR application, which in turn can provide important information for teachers who are considering investing resources and time into tailoring and implementing VR into their classrooms.
CURRICULUM AND ENVIRONMENT OF STUDY
Physical therapists play an important role in the screening of patients with cervical spine conditions. Screening for potential cervical instability arising from traumatic, systemic, or congenital conditions is of vital importance to patients with neck injuries and is used to rule out serious neck pathology requiring further investigation (Mathers et al., 2011). In Canadian MPT training programs, students are trained to assess ligament integrity, which is included in every upper quadrant assessment. Testing of the transverse ligament via the transverse ligament test/ anterior shear stress test is an example of one of several ligament tests for the cervical spine. If a deficit in the ligament integrity is found, the patient must be referred to a physician immediately. Conducting a client assessment, correctly identifying urgent health conditions that require immediate attention, and taking appropriate action are essential competencies and entry-to-practice milestones for physical therapy students (National Physiotherapy Advisory Group, 2017).
In the MPT program at our institution, the manual skill of testing and interpreting the transverse ligament stress test is taught in the first year of the program. Students complete their gross anatomy course three months prior to this point in the curriculum. At this early stage, the learning objectives related to the transverse ligament stress test focus on the “set,” “guided response,” and “mechanism” levels of psychomotor domain on Bloom’s Taxonomy (Clark, 1999; Simpson, 1966). Our students are first provided with relevant theory regarding the test, including the indications, signs, and symptoms of positive tests, as well as the testing techniques. Next, the instructors provide the students with a demonstration of the test on a plastic model of the cervical spine and on a student volunteer at the front of the classroom. Following this demonstration, students are paired with other classmates to practice these tests while instructors circulate in the lab to provide guidance on palpation skills, accurate landmarking, handling technique, and clinical reasoning that should occur during a successful stress test.
METHODOLOGY
This section is divided into two main parts. The first part outlines the development of a custom VR application learning tool that was guided by experiential learning theory and constructivist pedagogy. The second part outlines the assessment of the student experiences with the custom tool, as well as their experiences with a commercial anatomy software that is widely used around the world. The custom software (Luxsonic Technologies Inc., n.d.) allowed a very focused experience specific to manual therapy handling needs for MPT students. The commercial software (3D Organon, n.d.) was included in this study so that students could experience a commercial grade platform specifically used for anatomy learning and compare that to the custom software experience.
Virtual Reality Application Development Based on Experiential Learning Theory and Constructivist Pedagogy
Our academic team was comprised of faculty and instructors from different health professions (i.e., physical therapy, nursing, and speech language pathology) who share a common vision and passion for developing teaching tools to enhance the learning experience of students. Virtual reality learning experts from Luxonic Technologies Ltd (n.d.) developed the custom software. The team selected the cervical spine as a focus for this project, as this is an anatomic area that could be expanded on in future interprofessional projects, with discipline-specific learning skills for students.
A constructivist learning perspective and experiential learning theory, which are common educational underpinnings for many physical therapy curricula, guided design and development of the VR application (Qasem, 2015). The learning expectations corresponding to the “set,” “guided response,” and “mechanism” levels of the psychomotor domain of Bloom’s Taxonomy helped to specify learning objectives appropriate for students at this point in their training (Clark, 1999; Simpson, 1966). We followed the process recommended by Hanson and Shelton (2008) for the design and development of VR for instructional purposes. Key activities that took place, including each step and the educational theories that guided decisions, are reviewed here in more detail.
ARTICULATION OF VR APPLICATION EXPECTATION
Expectations for how the VR application would enhance the learning outcomes for the MPT students compared to the traditional methods of teaching of the ligament test were discussed and outlined as a team. The key expectations were as follows:
-
Opportunity for self-paced review of the craniovertebral anatomy in 3D.
The application would allow students to manipulate the anatomy and view structures in multiple viewpoints and positions relevant to understanding the transverse ligament stress test. The constructivist principles used to guide this process were as follows:
- Skills promotion and subject mastery are fostered through self-guided learning and rich exploration (Dewey, 1916).
- Prior learning experiences and views serve as a foundation to develop new knowledge (Phillips, 1995).
-
Opportunity for guided training in a low-stakes, safe, and realistic environment. The application would allow for gradual progression as learners moved from beginner to intermediate levels (i.e., observation of the skills; imitation of the skills through guided steps with visual, auditory, and tactile feedback; gradual removal of visual cues; and clinical reasoning and reflective questions). This process was guided by the constructivist principle that the learner takes on an active role (Dewey, 1916). We considered the following experiential learning principles: students should have the opportunity to observe and practice in a real-world setting, the opportunity to learn from mistakes and successes, and the opportunity to take initiative, reflect, and make decisions (Kolb, 1984; McCarthy, 2010).
FAMILIARIZATION WITH VR
In conjunction with Step 1, outlined above, our team investigated and trialed different commercial and custom VR applications (3D Organon, n.d.; Sharecare Virtual Reality (VR)—Making Health Visual, n.d.; Banow &Maw, 2020). This process allowed us to better understand what might be feasible with VR and what limitations there might be for the learning experience and outcomes we envisioned. We also considered the implications of the use of controllers versus haptic gloves in better mimicking the hand position used for the ligament stress test, as haptic gloves were not yet ready for use in this manner at the time of this pilot.
We did not find a commercial anatomy VR software that was able to provide the level of focused review of the CV anatomy in 3D that was the impetus for the first key expectation (a.) outlined above.
EVALUATION OF DESIGN CONSIDERATIONS
The research team worked closely with an industry partner over several months on this step. Meetings focused on design considerations, such as how we could set up the virtual work to best promote experiential learning; how students would receive visual, auditory, and tactile feedback; and how to create an experience as close as possible to a hands-on clinical experience.
Initial versions of the software were tested by two experienced orthopedic physiotherapy instructors with over 20 years of MPT teaching experience (Kendra Usunier and Soo Kim). After independently using the VR software, the instructors provided feedback to the Luxonic Technologies developers. Feedback focused on details that would help make the immersive experience as anatomically and technically similar to a real-life scenario as possible (i.e., fine tuning of hand placement, the degree of hand movement needed, the verbal and written communication provided to students during the application, and the clinical reasoning that occurs during the technique). The process was iterative.
EVALUATION OF BUDGET AND RESOURCE
We discussed which design considerations to prioritize based on our available funding. We then developed a timeline to purchase equipment with potential funding and to seek additional funding through grant opportunities to ensure development and evaluation of the custom application.
Figure 1 provides an overview of the key features of the VR application.
Figure 1
Key Features of Custom VR Application
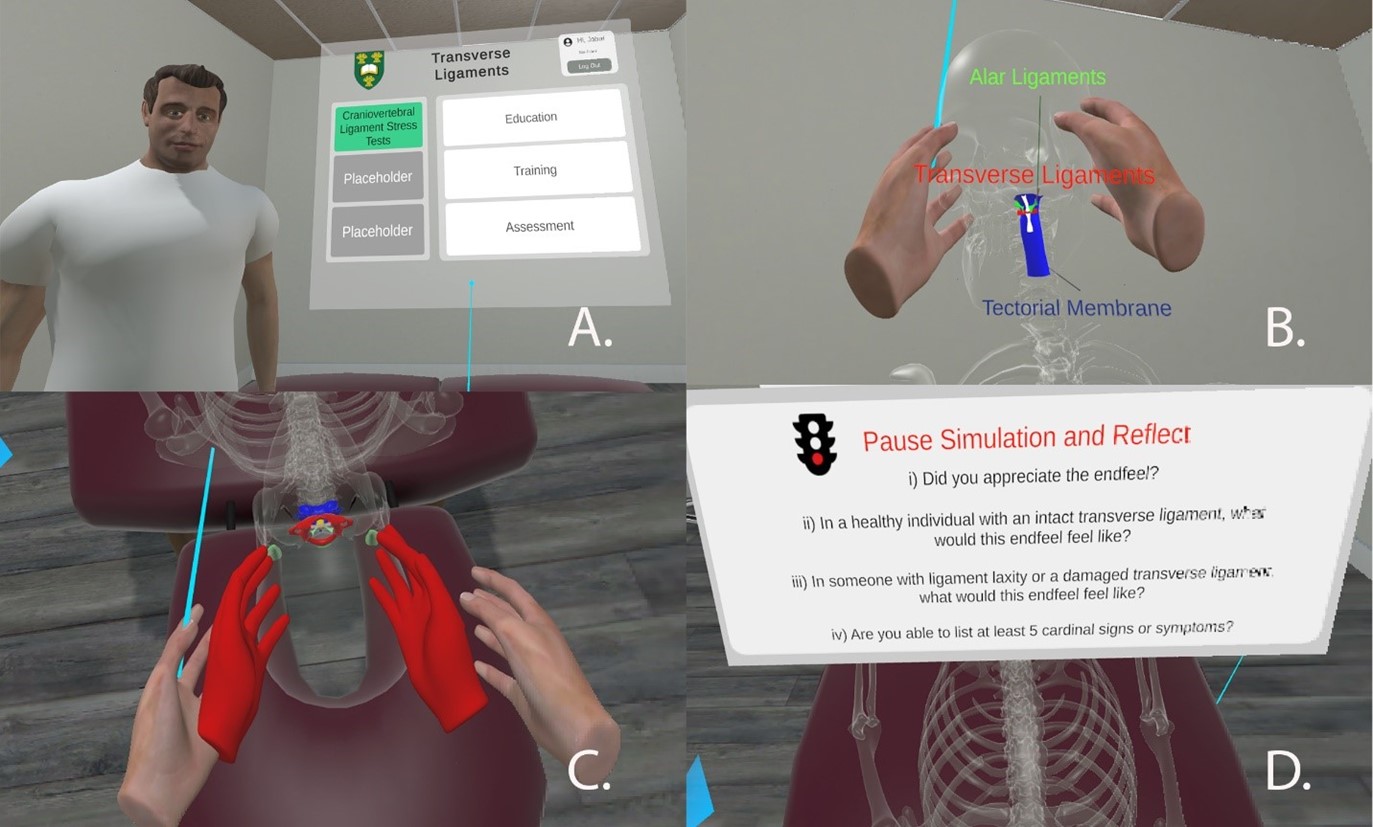
-
A clinic assessment room was used to develop a realistic immersive environment. A male avatar represents the virtual “client” in the experience. Following orientation to VR, students are presented with three modes: education, training, and assessment. (Note: Placeholders were created for the addition of other ligament tests in the future.) For our pilot study, our students experienced the education and training modes. The assessment mode was not completed for this version of the software.
-
The education mode provides students with the opportunity for self-paced review of the CV anatomy. Students can view different anatomical structures with the “client” in different positions (lying, standing, or sitting) and can view different layers of the anatomy (skin, muscles, and bone). Students can handle the “client” and move them around to view structures in different orientations.
-
The training mode provides students with the opportunity to practice the transverse ligament stress test and facilitates the various levels of student learning. There is a “walkthrough” option for beginner learners, which provides students with practice as they follow and imitate the demonstration, experiencing visual, auditory, and tactile feedback. Visual (colour-changing hands) and tactile feedback (vibration) acknowledge correct hand positioning.
-
When the task is done correctly, a prompt appears that guides the student through the clinical reasoning and facilitates reflection.
Note: Text correlates with labelled parts of the figure (A, B, C, and D) and describes education and training modes within the VR experience.
ASSESSMENT OF STUDENT LEARNING EXPERIENCES WITH VR APPLICATIONS
Participants
There were eight MPT student participants in this study. Seven were 20 to 30 years old, and one was over age 30. All volunteer participants were female. One senior-level MPT student was recruited through an email advertisement asking for participants in a beta-test experience of the custom software VR learning tool. This student had previously completed the orthopedic course that introduces transverse ligament stress testing through didactic and hands-on practical learning. Following software modifications resulting from the senior student’s feedback, seven students from the introductory musculoskeletal course were recruited through email and in person. One of the researchers who was not involved in instruction or assessment of students during the period of the study attended class to talk about the project, provide information, and answer questions for potential volunteer participants. All participants provided written consent prior to participation. Institutional ethics approval for this research was obtained through the institution’s Behavioural Research Ethics Board. The sample size of this project was reduced from the anticipated plan due to multiple delays related to COVID-19 restrictions.
Methods
This study followed a qualitative research design. In order to identify participant demographics, history of health and medical conditions, and prior experience with cervical ligamentous testing and VR systems, participants were asked to complete three pre-study questionnaires prior to the VR experience. Participants completed the questionnaires and consent forms using Survey Monkey.
Semi-Structured Interview. A semi-structured interview was completed with participants within one week of beta and pilot testing. Questions are included in Appendix A. There were nine open-ended questions, eight focusing on the custom VR learning experience and one on the experience in comparison to the commercial software. The questions used in the semi-structured interviews were guided by the constructs of the technology acceptance model (TAM). Semi-structured interview questions were reviewed by two researchers with extensive experience in qualitative research. Questions were assessed for clarity and content validity.
Beta Testing. The senior student participated in experiencing both the custom software and the 3D Organon commercial software (n.d.). She provided feedback during these VR learning sessions and completed a semi-structured interview following participation to describe her experience. This information was utilized to enhance the custom software experience and learner comfort prior to the pilot, as well as to refine instructions for students and the process for the intervention.
Pilot Testing of VR Protocol. Participants were randomly assigned to experience either the custom or commercial software on one occasion and the other software seven days later. Both experiences lasted 20–30 minutes. A researcher who was not involved in class instruction or evaluation was present throughout the intervention on both occasions. She provided an orientation to participants on the software and procedures, and she answered any questions that arose during the learning experience. Semi-structured interviews were completed following the second experiential VR session.
Data Analysis. Descriptive analysis was conducted for the pre-testing questionnaires. Semi-structured interviews were audio recorded and transcribed by a researcher. Iterative qualitative analysis followed processes recommended by Vaismoradi et al. (2013) and Braun and Clarke (2021), including familiarization with data, and open and axial coding to identify themes and connections between experiences. An experienced qualitative researcher developed codes, which were verified by a second researcher with specific content expertise in the teaching of orthopedic MPT courses. The researchers conducted independent analyses. Final decision making on themes occurred through consensus.
RESULTS
Of the eight student participants, five reported previous experience with VR for entertainment purposes. No participants had medical histories that would prevent them from participating, and none had experienced dizziness or vertigo in the previous year. Four had glasses that would be worn during VR, and one wore glasses that were removed during VR. All eight students reported a history of pain during previous hands-on partnered lab experiences with cervical spine palpation and ligamentous stress testing. This included localized pain, mild-to-moderate muscle stiffness, and mild headache. All students reported palpation to be the most difficult component of this complex manual skill, with 7 of 8 reporting that the ability to appreciate ligamentous end feel in a stress test was challenging, and 6 of 8 indicating that confidence as well as knowing how much force to exert during the ligamentous stress test were challenging components.
The beta-test participant (senior student) indicated that her back became sore due to bending forward for a prolonged period to complete the training application. The treatment bed in the custom VR application was stationary and, as a result, could not be repositioned higher to facilitate optimal body mechanics for the student clinician. In response to this concern, the software developer modified the custom software to allow a participant to raise and lower the virtual treatment bed to ensure optimal body mechanics. Students spent an average of 23.7 minutes with the education and training modes in the custom software and 22.7 minutes with the commercial software.
Experience with Virtual Reality — Themes
Themes were inductive in nature and emerged from the thematic analysis. Qualitative themes resulting from semi-structed interviews included 1) learning in a stimulating low-stakes environment, 2) recommendations to enhance learning and experience with VR, and 3) challenges.
LEARNING IN A STIMULATING LOW-STAKES ENVIRONMENT
Participants reported that the custom software assisted with solidifying and helping them to understand the ligamentous stress testing skill and visualization of anatomy. The ability to practice repeatedly without fear of hurting a partner aided in better understanding the skill. Specific to the anatomy education application, one participant reported, “It was really helpful to see the actual ligament while you are stressing it, like just being able to see inside the body as opposed to with just regular people, it helped with the visualization.” Another stated, “For me it was helpful that I could see ligaments and structures because once I can imagine something I can understand what I am doing a lot better.” The participants also appreciated the ability to learn with different layers (skin, muscle, bone). One participant explained that this experience was “really good for visualization. [You] can peel back the layers (skeleton, muscle, or full patient) and have an idea of what you are doing internally, which you don’t have in lab.”
Regarding the guided training in the custom software, a participant said, “with the cues when you are on the right spot, it will vibrate and that was really helpful for me.” Another participant indicated appreciating that “no one is complaining that you are poking them,” and a third said, “You can just go and train and not worry about hurting someone.” Overall, participants described the custom software as being “awesome, would recommend it to others,” “neat,” “really cool,” “quite immersive,” and “easy to use.”
The students appreciated the commercial software as well. As one participant explained,
I liked that it [the commercial software] had the different layers—muscle, bone, nerves. You could take off a part of the skull to see the ligament, could take off certain pieces. That one was just a little bit more developed, and it was a little more helpful in terms of studying.
In comparison to the custom software, one participant reported,
I liked that one [the commercial software] to get in and visualize what you are doing a bit more. [I] liked the custom for the testing. You could actually do the hand placements for testing, but I liked to be able to get a better idea of structures … and everything posted [in the commercial software] so you could read about the actions and whatnot, being able to associate them when it’s right in front of you.
RECOMMENDATIONS TO ENHANCE LEARNING AND EXPERIENCE WITH VR
This theme defined areas that students felt could be added or improved to increase the value of the custom experience. They overwhelmingly recommended adding other craniovertebral ligament tests. As one student explained, it “would be good to have it for other ligament tests also, to understand the motion of your hands” and added that “more information about the test and reminder about cardinal signs” would improve the experience. The students also recommended increased play opportunity with anatomy, such as “muscles and vessels to take apart and look at as a whole structure.” Participants believed it would be helpful to use their hands with haptic gloves as well as to be able to move the VR patient’s limbs, etc. They also felt that the commercial software (3D Organon, n.d.) would be very beneficial in their program for learning anatomy in general due to the high degree of development in the software. For example, one participant noted that “you could take off a part of the skull to see the ligament, could take off certain pieces,” and it was “nice because [there was] so much to it and so many layers, was nice to be able to look at skeletal muscle, isolate it, look at blood flow.”
CHALLENGES
Some challenges reported by participants included some disorientation and sense of difficulty moving around. Participants also noted that the handsets were a bit difficult, especially having to navigate buttons on the handsets during the experience. Two participants reported some difficulty focusing their eyes during the experience.
DISCUSSION
This SoTL study presented the design and evaluation of a custom VR application and aimed to answer the research question: What is the experience of MPT students with a VR learning platform for transverse ligamentous stress testing in the upper cervical spine? The study also provided pedagogical insights so that VR technology can be integrated into curricula and programs facing similar challenges with practical hands-on skill instruction. Pilot test results showed that students found the custom VR application to be beneficial for their learning of the transverse ligament stress test and that it could mitigate drawbacks associated with practice on peers—namely discomfort in form of localized neck pain, mild to moderate muscle stiffness, and headaches.
Our team created a novel VR application to enhance learning of the upper cervical spine ligamentous stress tests and assessed students’ experiences with the innovative VR learning tool. Previous VR research on advances and implementation in the classroom has informed approaches for VR development and common challenges educators face with various educational applications (Hansen & Shelton, 2008; Rizzo et al., 2004). There is also a growing body of SoTL literature that informed us about research methods that can be useful in studying the impact of VR on student learning experiences and teaching practices (Jiang et al., 2022; Kyaw et al., 2019; Mao et al., 2021; Zhao et al., 2020). In addition, the principles for good SoTL practice outlined by Felten (2013) helped us to plan, evaluate, and reflect on our study. In contrast to many of the VR studies published in health science education, however, our study provides a novel example and insights on the pedagogical considerations specific to VR and psychomotor skill development, which is not widely covered in the SoTL literature and will have an important impact on other professional educators seeking innovative methods to teach practical/hands-on competencies. Data from the semi-structured interviews support the educational benefits and usefulness of our VR application. Overall, students’ experiences with the VR application were positive.
In keeping with experiential and constructivist principles, students appreciated the opportunity in the custom VR experience for self-guided visualization of the relevant craniovertebral anatomy. They consistently reported the value and usefulness of visualizing the ligament in a manner that facilitated better understanding of the skills required to complete the transverse ligament stress test. Students reported their appreciation of the ability to visualize and experience the different layers of anatomy (i.e., skin, muscle, or bone) and perceived this as very helpful in making connections with the hands-on skills in a way they would not be able to in the traditional lab.
Our students’ reported experiences similar to those identified in other studies focusing on VR anatomy (Moro et al., 2017). Although students noted that the commercial anatomy VR software offered more detail and was “more developed” than our custom VR application, they acknowledged that the custom experience was more directed to what they were doing in the classroom. This finding seems to support and validate our intent for designing our own anatomy tool, which was to provide a focused review of relevant anatomy in views that would best facilitate learning of the transverse ligament stress test. Inclusion of an anatomy review section directly relevant to the clinical skill at hand is also commonly seen with other VR applications focusing on training surgical skills, such as the Osso VR hands-on surgical training platform (Blumstein et al., 2020). In a constructivist paradigm, a learner’s previous knowledge is used to construct new knowledge; thus, future researchers wishing to integrate VR for clinical skills training may want to facilitate bridging the gap between students’ knowledge and real-life clinical problem solving with an opportunity to review the relevant anatomy, if applicable, as we have demonstrated.
For both the “education” and “training” modes, student users enjoyed learning in a low-stakes environment. Using our custom VR application, students could take as much time as they wanted with different modes, and repetitive practice of the skills was allowed with visual, tactile, and auditory guidance and feedback. One of the key elements of experiential learning and a low-stakes learning environment is that students are given the opportunity to try, to make mistakes, and to learn from those mistakes with little or no negative consequence. Trial and error coupled with insights from formative feedback in this type of learning environment have been found to improve students’ learning (Butler, 1987; Narciss & Huth, 2004; Shute, 2008; Thorndike, 1932). Although the students in our study were given one session to use the custom VR application, our long-term goal is to have it available for all students for repeated use and distributed practice throughout the curriculum. Extensive evidence exists to show that distributed practice compared to massed practice can lead to more durable learning (Roediger, 2013).
In our study, all students reported a history of experiencing localized neck pain in the traditional lab setting, when having the transverse ligament stress tests skill practiced on them. As such, it was not surprising to see several student comments within the theme “learning in a stimulating low-stakes environment” stating how they appreciated the ability to practice and learn without fear of causing harm to a peer partner. One of the key motivations for our training application, and that of many other VR simulators focusing on psychomotor skills, is that students can maximize their clinical practice within a real-life application while minimizing harm or risk to patients or peer training partners (Zhao et al., 2020; Zitzmann et al., 2020). This also allows additional options for student practice when lab time is limited in the curriculum.
Despite VR’s ability to encourage learning across many domains (Izard et al., 2018), there is a notable gap in VR development and use for training physical therapy students compared to other health professions. In the National Study of Excellence and Innovation in Physical Therapist Education, there was a call for transformative changes that can be informed by medical and nursing education innovations (Jensen, 2006). With the rapid growth of VR in education and a precedent from other health professions, we hope our project helps stimulate greater exploration and discussion of specific pedagogies for increased VR use to advance teaching and learning practices in physical therapy programs.
Limitations
The sample size for this SoTL project was lower than we had anticipated. There are several potential reasons for this: 1) the pilot project relied entirely on student participation, which is a limitation noted in SoTL research (Divan et al., 2017), 2) the course load of the MPT program when this project occurred was extremely heavy, so students may have felt too busy to participate, and 3) students may not have seen the value in volunteering because they were not involved in the planning and development phases. Felten (2013) notes that partnering with students in inquiry is becoming an important component in SoTL. Another limitation specific to the training of the clinical skill itself was that haptic gloves were not available when this project was undertaken. The hand controllers do not mimic the exact hand postures that would be utilized in this skill set, and participants reported some awkwardness in that respect. This is a barrier that would require haptic gloves to overcome. Finally, this project was delayed on two occasions due to COVID-19 restrictions. As a result, we proceeded with a reduced number of participants and only as a pilot program, with the intention of expanding the project post-COVID.
Future Directions
Several areas for future research were identified as a result of this study. Students recommended the addition of training for the other ligaments in the VR experience, which was a goal that our team had previously identified. Future research will focus on the addition of other craniovertebral ligaments and expansion of the training to include a head and upper quadrant scan for interprofessional health providers. We will also include the use of haptic gloves, which will provide a more realistic learning experience. We have learned with the COVID-19 pandemic that we need to adapt our teaching methods to include additional options for distance and virtual learning, and our application can serve as a platform for these different modes of learning. Although we do not believe VR would replace face-to-face instruction of these skills, this pilot suggests that it provides a worthwhile addition to learning in this area and allows repeated and distributed practice without the barrier of provoking pain or headache in one’s partner. Finally, this project has the potential to be modified and scaled up for collaboration with other health science and hands-on professions and programs.
CONCLUSION
Our interdisciplinary team has developed a VR learning application that focuses on the learning of craniovertebral anatomy practical skills of testing the transverse ligament, which is a critical safety test for assessing stability of the neck and head. This application can be used not only to train entry-level physical therapists, but also for continuing learning by experienced therapists and by other health professionals with training needs involving the craniovertebral region. In addition, the transverse ligament is but one of several ligament tests of the neck that can be expanded upon within this custom VR application.
How to Cite
Lovo, S., Leidl, D., Usunier, K., Paslawski, T., Wesolowski, M., Puri, A., Caron, V., &Kim, S. (2024). Development and assessment of learners’ experiences with a virtual reality learning platform: Constructivist and experiential learning pedagogies in Master of Physical Therapy curriculum. Imagining SoTL, 4(1), 39–61. https://doi.org/10.29173/isotl682
Author Biography
Stacey Lovo (stacey.lovo@usask.ca) is a physical therapist and Assistant Professor in the School of Rehabilitation Science at University of Saskatchewan. Her research focuses on culturally responsive healthcare and the use of technologies to enhance access to healthcare services and education.
Don Leidl is an Assistant Professor at the University of New Brunswick Faculty of Nursing. His clinical background is in adult acute psychiatry and psychiatric emergency services for adults and adolescents. His research focuses on the use of immersive virtual reality technology in nursing and health sciences education.
Kendra Usunier is Program Director for Continuing Education in Rehabilitation Science at the University of Saskatchewan and teaches in the Master of Physical Therapy program. Her clinical background is in orthopedics and women’s health, and she has advanced credentials as a fellow of the Canadian Academy of Manipulative Physiotherapy.
Teresa Paslawski is an Associate Professor in the College of Medicine, University of Saskatchewan. She is a speech pathologist with a PhD in neuroscience. She has worked clinically, primarily in acute care, and taught in speech pathology and education. Her research interests include clinical education, interprofessional collaboration, and neurological disorders.
Mike Wesolowski is the founder of Luxsonic Technologies, a company on a mission to improve global access to healthcare using immersive technology. He is an Adjunct Professor of Medical Imaging at the University of Saskatchewan and a passionate advocate of using “tech for good.”
Arjun Puri is the Senior Digital Health Strategist at the Data Intelligence for Health Lab, Department of Cardiac Sciences at the University of Calgary. Arjun specializes in advancing innovative healthcare solutions into clinical practice. His areas of expertise include digital health, immersive technologies, and health informatics.
Valerie Caron is a physical therapist and is completing her PhD in neurorehabilitation and animal-assisted interventions. She teaches in the Master of Physical Therapy program and has an interest in innovative approaches to healthcare and education of healthcare professionals.
Soo Kim is a Professor at the School of Rehabilitation Science, University of Saskatchewan. She is a clinical anatomist and physical therapist, and her research program investigates muscle architecture and function in response to pathology, surgery, and rehabilitation. She is passionate about designing innovative teaching methods to enhance student learning.
ACKNOWLEDGEMENTS AND CONFLICT OF INTEREST DISCLOSURES
The authors would like to thank Ryan Banow, Program Development Specialist at the Gwenna Moss Centre for Teaching and Learning, University of Saskatchewan, for consultation and guidance in SoTL project design methods. We would also like to thank Joy Richards, Continuing Education in Rehabilitation Science, for designing the Survey Monkey questionnaire. This project was funded from multiple sources: SoTL grants through the Gwenna Moss Centre for Teaching and Learning and the Jane and Ron Graham Centre for the Scholarship of Teaching and Learning, University of Saskatchewan, faculty start-up funds, as well as a McClelland Fund through the College of Medicine, University of Saskatchewan, for the purchase of VR equipment. Part of the funding received went to the development of software by Luxonic Industries Ltd.
References
3D Organon [Computer software]. (n.d.). https://store.3dorganon.com/en/?controllerUri=index&gclid=
CjwKCAiA85efBhBbEiwAD7oLQBE7yAeqPlDWRuZP5bLTrL-zt7qEbiUcSD9w5gGNsVDrvtjcqO9dlxoCleAQAvD_BwE
Andresen, L., Boud, D., & Cohen, R. (2020). Experience-based learning. In G. Foley (Ed.), Understanding adult education and training (2nd ed., pp. 225–239). Routledge. https://doi.org/10.4324/9781003118299-22
Banaszek, D., You, D., Chang, J., Pickell, M., Hesse, D., Hopman, W. M., Borschneck, D., & Bardana, D. (2017). Virtual reality compared with bench-top simulation in the acquisition of arthroscopic skill: A randomized controlled trial. Journal of Bone and Joint Surgery, 99(7), e34. https://doi.org/10.2106/JBJS.16.00324
Banow, R., & Maw, S. (2020). Pilot study results from using TrussVR© to learn about basic trusses. 2020 ASEE Virtual Annual Conference Content Access Proceedings, 35055. https://doi.org/10.18260/1-2--35055
Blumstein, G., Zukotynski, B., Cevallos, N., Ishmael, C., Zoller, S., Burke, Z., Clarkson, S., Park, H., Bernthal, N., & SooHoo, N. F. (2020). Randomized trial of a virtual reality tool to teach surgical technique for tibial shaft fracture intramedullary nailing. Journal of Surgical Education, 77(4), 969–977. https://doi.org/10.1016/j.jsurg.2020.01.002
Braun, V., & Clarke, V. (2021). Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern‐based qualitative analytic approaches. Counselling and Psychotherapy Research, 21(1), 37–47. https://doi.org/10.1002/capr.12360
Brinkmann, C., Fritz, M., Pankratius, U., Bahde, R., Neumann, P., Schlueter, S., Senninger, N., & Rijcken, E. (2017). Box- or virtual-reality trainer: Which tool results in better transfer of laparoscopic basic skills?—A prospective randomized trial. Journal of Surgical Education, 74(4), 724–735. https://doi.org/10.1016/j.jsurg.2016.12.009
Butler, R. (1987). Task-involving and ego-involving properties of evaluation: Effects of different feedback conditions on motivational perceptions, interest and performance. Journal of Educational Psychology, 79(4), 474–482.
Clark, D. (1999). Bloom’s Taxonomy: The psychomotor domain. http://www.nwlink.com/~donclark/hrd/bloom.html
Codd, A. M., & Choudhury, B. (2011). Virtual reality anatomy: Is it comparable with traditional methods in the teaching of human forearm musculoskeletal anatomy? Anatomical Sciences Education, 4(3), 119–125. https://doi.org/10.1002/ase.214
Davis, A. J., Davidson, B., Hirschfield, M., Lauri, S., Lin, J. Y., Norberg, A., Phillips, L., Pitman, E., Shen, C. H., Vander Laan, R., Zhang, H. L., & Ziv, L. (1993). An international perspective of active euthanasia: Attitudes of nurses in seven countries. International Journal of Nursing Studies, 30(4), 301–310. https://doi.org/10.1016/0020-7489%2893%2990102-Z
Davis, F. D. (1989). Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Quarterly, 13(3), 319–340. https://doi.org/10.2307/249008
Dewey, J. (1916). Democracy and education: An introduction to the philosophy of education. MacMillan.
Di Vece, C., Luciano, C., & De Momi, E. (2021). Psychomotor skills development for Veress needle placement using a virtual reality and haptics-based simulator. International Journal of Computer Assisted Radiology and Surgery, 16(4), 639–647. https://doi.org/10.1007/s11548-021-02341-0
Divan, A., Ludwig, L., Matthews, K., Motley, P., & Tomljenovic-Berube, A. (2017). Survey of research approaches utilized in the Scholarship of Teaching and Learning publications: A systematic literature review. Teaching & Learning Inquiry, 5(2), 1–16. https://doi.org/10.20343/teachlearninqu.5.2.3
Estai, M., & Bunt, S. (2016). Best teaching practices in anatomy education: A critical review. Annals of Anatomy—Anatomischer Anzeiger, 208, 151–157. https://doi.org/10.1016/j.aanat.2016.02.010
Felten, P. (2013). Principles of good practice in SoTL. Teaching & Learning Inquiry, 1(1), 121–125. https://doi.org/10.20343/teachlearninqu.1.1.121
Hansen, K., & Shelton, B. (2008). Design and development of virtual reality: Analysis of challenges faced by educators. Educational Technology and Society, 11(1), 118–131.
Hartstein, A., Verkuyl, M., Zimney, K., Yockey, J., & Berg-Poppe, P. (2022). Virtual reality instructional design in orthopedic physical therapy education: A mixed-methods usability test. Simulation and Gaming, 53(2), 111–134. https://doi.org/10.1177/10468781211073646
Huang, H.-M., & Liaw, S.-S. (2018). An analysis of learners’ intentions toward virtual reality learning based on constructivist and technology acceptance approaches. The International Review of Research in Open and Distributed Learning, 19(1), 1–25. https://doi.org/10.19173/irrodl.v19i1.2503
Huang, H.-M., Rauch, U., & Liaw, S.-S. (2010). Investigating learners’ attitudes toward virtual reality learning environments: Based on a constructivist approach. Computers & Education, 55(3), 1171–1182. https://doi.org/10.1016/j.compedu.2010.05.014
Izard, S. G., Juanes, J. A., García Peñalvo, F. J., Estella, J. M. G., Ledesma, M. J. S., & Ruisoto, P. (2018). Virtual reality as an educational and training tool for medicine. Journal of Medical Systems, 42(3), 1–5. https://doi.org/10.1007/s10916-018-0900-2
Jensen, M. P. (2006). Review of measures of neuropathic pain. Current Pain and Headache Reports, 10(3), 159–166. https://doi.org/10.1007/s11916-006-0041-z
Jiang, H., Vimalesvaran, S., Wang, J. K., Lim, K. B., Mogali, S. R., & Car, L. T. (2022). Virtual Reality in medical students’ education: Scoping review. JMIR Medical Education, 8(1), e34860. https://doi.org/10.2196/34860
Judd, D. L., Kelly, B., & Corral, J. (2021). Using Virtual Reality for movement system examination in a Doctor of Physical Therapy curriculum. Journal of Physical Therapy Education, 35(4), 324–329. https://doi.org/10.1097/JTE.0000000000000204
Kolb, D. (1984). Experiential learning: Experience as the source of learning and development. Prentice Hall.
Kyaw, B. M., Saxena, N., Posadzki, P., Vseteckova, J., Nikolaou, C. K., George, P. P., Divakar, U., Masiello, I., Kononowicz, A. A., Zary, N., & Tudor Car, L. (2019). Virtual Reality for health professions education: Systematic review and meta-analysis by the Digital Health Education Collaboration. Journal of Medical Internet Research, 21(1), e12959. https://doi.org/10.2196/12959
Luxsonic Technologies Inc. [Computer software]. (n.d.). https://luxsonic.ca/
Mao, R. Q., Lan, L., Kay, J., Lohre, R., Ayeni, O. R., Goel, D. P., & de SA, D. (2021). Immersive virtual reality for surgical training: A systematic review. Journal of Surgical Research, 268, 40–58. https://doi.org/10.1016/j.jss.2021.06.045
Mathers, K. S., Schneider, M., & Timko, M. (2011). Occult hypermobility of the craniocervical junction: A case report and review. Journal of Orthopaedic & Sports Physical Therapy, 41(6), 444–457. https://doi.org/10.2519/jospt.2011.3305
McCarthy, M. (2010). Experiential learning theory: From theory to practice. Journal of Business, 8(5), 131–140.
Miller, R. (2000). Approaches to learning spatial relationships in gross anatomy: Perspective from wider principles of learning. Clinical Anatomy, 13(6), 439–443. https://doi.org/10.1002/1098-2353(2000)13:6<439::AID-CA8>3.0.CO;2-X
Moro, C., Štromberga, Z., Raikos, A., & Stirling, A. (2017). The effectiveness of virtual and augmented reality in health sciences and medical anatomy: VR and AR in health sciences and medical anatomy. Anatomical Sciences Education, 10(6), 549–559. https://doi.org/10.1002/ase.1696
Narciss, S., & Huth, K. (2004). How to design informative tutoring feedback for multimedia learning. In H. M. Niegemann, D. Leutner, & R. Brünken (Eds.), Instructional design for multimedia learning (pp. 181–195). Waxmann.
National Physiotherapy Advisory Group. (2017). NPAG competency profile for physiotherapists in Canada. https://peac-aepc.ca/pdfs/Resources/Competency%20Profiles/Competency%20Profile%20for%20PTs%202017%20EN.pdf
Nicholson, L. L., Reed, D., & Chan, C. (2016). An interactive, multi-modal anatomy workshop improves academic performance in the health sciences: A cohort study. BMC Medical Education, 16(1), 1–9. https://doi.org/10.1186/s12909-016-0541-4
Phillips, D. C. (1995). The good, the bad, and the ugly: The many faces of constructivism. Educational Researcher, 24(7), 5–12. https://doi.org/10.3102/0013189X024007005
Qasem, M. (2015). Constructivist Learning Theory in physiotherapy education: A critical evaluation of research. Journal of Novel Physiotherapies, 5(2), 1–3. https://doi.org/10.4172/2165-7025.1000253
Rahm, S., Wieser, K., Bauer, D. E., Waibel, F. W., Meyer, D. C., Gerber, C., & Fucentese, S. F. (2018). Efficacy of standardized training on a virtual reality simulator to advance knee and shoulder arthroscopic motor skills. BMC Musculoskeletal Disorders, 19(1), 1–7. https://doi.org/10.1186/s12891-018-2072-0
Rizzo, A., Cohen, I., Weiss, P., Kim, J., Yeh, S., Zali, B., & Hwang, J. (2004). Design and development of virtual reality based perceptual-motor rehabilitation scenarios. Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (pp. 4852–4855). https://doi.org/10.1109/IEMBS.2004.1404342
Roediger, H. L. (2013). Applying cognitive psychology to education: Translational educational science. Psychological Science in the Public Interest, 14(1), 1–3. https://doi.org/10.1177/1529100612454415
Rourke, S. (2020). How does virtual reality simulation compare to simulated practice in the acquisition of clinical psychomotor skills for pre-registration student nurses? A systematic review. International Journal of Nursing Studies, 102, 1–7. https://doi.org/10.1016/j.ijnurstu.2019.103466
Sharecare Virtual Reality (VR)—Making Health Visual. [Computer software]. (n.d.). https://www.sharecare.com/pages/vr
Shute, V. J. (2008). Focus on formative feedback. Review of Educational Research, 78(1), 153–189. https://doi.org/10.3102/0034654307313795
Simpson, E. (1966). The classifications of educational objectives, psychomotor domain. University of Illinois. https://files.eric.ed.gov/fulltext/ED010368.pdf
Smith, S. N., & Crocker, A. F. (2017). Experiential learning in physical therapy education. Advances in Medical Education and Practice, 8, 427–433. https://doi.org/10.2147/AMEP.S140373
Sultan, L., Abuznadah, W., Al-Jifree, H., Khan, M. A., Alsaywid, B., & Ashour, F. (2019). An experimental study on usefulness of Virtual Reality 360° in undergraduate medical education. Advances in Medical Education and Practice, 10, 907–916. https://doi.org/10.2147/AMEP.S219344
Thorndike, E. (1932). The fundamentals of learning. Teachers College Press.
Turney, B. (2007). Anatomy in a modern medical curriculum. Annals of the Royal College of Surgeons of England, 89(2), 104–107. https://doi.org/10.1308/003588407X168244
Vaismoradi, M., Turunen, H., & Bondas, T. (2013). Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nursing & Health Sciences, 15(3), 398–405. https://doi.org/10.1111/nhs.12048
Zhang, L., Sankaranarayanan, G., Arikatla, V. S., Ahn, W., Grosdemouge, C., Rideout, J. M., Epstein, S. K., De, S., Schwaitzberg, S. D., Jones, D. B., & Cao, C. G. L. (2013). Characterizing the learning curve of the VBLaST-PT© (Virtual Basic Laparoscopic Skill Trainer). Surgical Endoscopy, 27(10), 3603–3615. https://doi.org/10.1007/s00464-013-2932-5
Zhao, J., Xu, X., Jiang, H., & Ding, Y. (2020). The effectiveness of virtual reality-based technology on anatomy teaching: A meta-analysis of randomized controlled studies. BMC Medical Education, 20(1), 1–10. https://doi.org/10.1186/s12909-020-1994-z
Zitzmann, N. U., Matthisson, L., Ohla, H., & Joda, T. (2020). Digital undergraduate education in dentistry: A systematic review. International Journal of Environmental Research and Public Health, 17(9), 1–23. https://doi.org/10.3390/ijerph17093269
Appendix
Tell us about your experience with the custom VR software for transverse ligament stress test.
Prompts: Did you enjoy the experience, or not? How many times were you able to use the VR? Which modes did you use (educational, practice, test mode)? What did you like the most/least?
Tell us about your experience with the commercial VR software and how that experience compared to the custom software.
Is there anything we could do or additions you would want to see made to the VR suite to improve the experience of the custom (transverse ligament) software?
Is there anything we could do or additions you would want to see made to enhance your learning of the transverse ligament stress test within the custom VR software?
Would you use VR software again to study cervical ligaments? Would you recommend this approach to learning to others? Why or why not?
What other MPT skills do you think would be useful to practice using VR?
Is there anything else you would like to tell us about or feedback you would like to provide?